
As part of the Migration, Health & Wellbeing in Context webinar series, the ACMS in partnership with Nuture4Youth, Global Health Research Group: GEMMS, the Cluster of Research Excellence (CoRE) in Migration & Health, and the Wits University School of Social Sciences is organising its second hybrid seminar, titled ‘Cities in Motion: Health, Violence & Crisis in SA’s Urban Worlds’.
Date: Tuesday 11 November 2025
Time: 10am – 11.30am (SAST)
In-person venue: African Centre for Migration & Society (ACMS) Seminar Room (see directions here)
Online: Zoom link here
Speakers:
– Diego Iturralde, Chief Director: Demography and Population Statistics, Statistics SA
– Silindile Mlilo, Xenowatch, ACMS, Wits
– Rebecca Walker, Collective Voices and ACMS, Wits
– Federica Duca, Johannesburg Crisis Working Group, PARI, Wits
– Lorena Nunez, School of Social Sciences, Wits
This webinar aims to facilitate an evidence-informed conversation about the intersecting and multi-level dynamics of migration and urbanisation and their impacts on population health and wellbeing in South Africa. Central to current debates is the need to focus on the structural and interpersonal violence – including that promoted by anti-foreigner vigilante groups – that remain defining features of life in many urban settings. It seeks to move beyond abstract policy debates by grounding discussion in real, tangible experiences and challenges, while also highlighting pathways toward more inclusive, equitable, and health-promoting urban futures.
Background
South Africa’s 2025 mid-year population estimates, highlight – once again – the impact that remaining the world’s most unequal country has on the health and wellbeing of everyone residing in the country. Numerous interlinked social and structural determinants of health – the result of the country’s history of segregation and pervasive inequality – negatively affect the health and wellbeing of all in the country. This is particularly acute in South Africa’s urban worlds where intersecting crises in the lived experiences of city residents continue to unfold.
Whilst at an aggregate level, urban spaces often have better health outcomes than rural areas, South Africa’s towns and cities hide the stark realities of inequity whereby marginalised urban poor groups face numerous drivers of poor health. As one of the most urbanised countries sub-Saharan Africa, over two-thirds of the South African population live in urban areas. As cities and towns grow – due to both natural growth and migration, they continue to grapple with the complex legacies of enduring apartheid-era spatial inequality, persistent socio-economic exclusion and uneven access to basic social services, including healthcare.
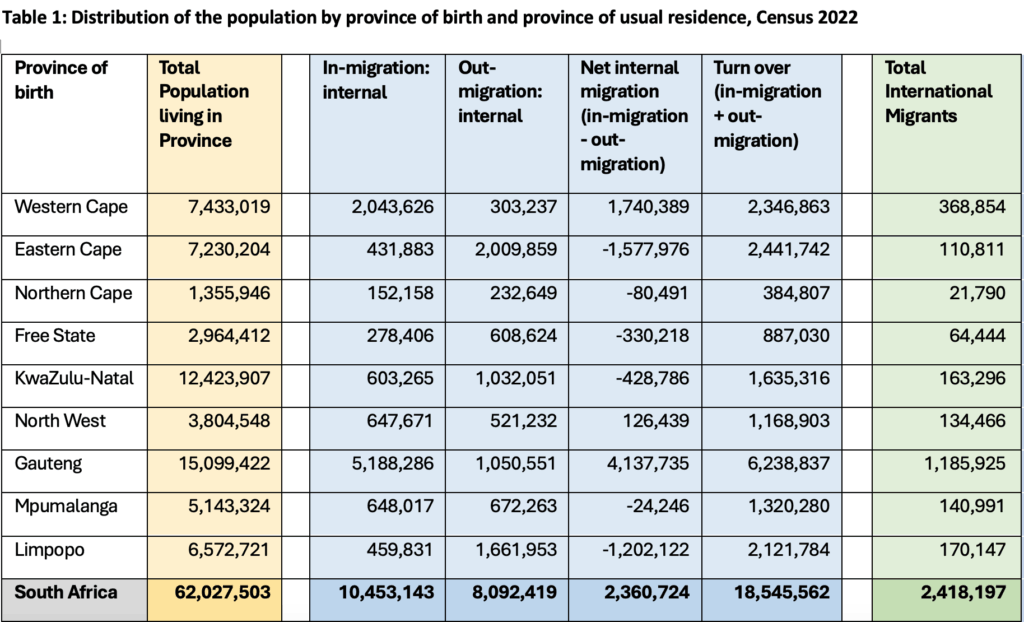
Despite popular misconceptions, there are just 2.5 million international migrants in the country, accounting for 4% of the South African population, with South Africa’s towns and cities remaining primary destinations for migrants from the Southern African region and beyond. But rarely spoken about are the 18 million people moving between provinces within South Africa – 29% of the total population (Table 1). Internal migration from rural to urban areas remains a key driver of urban growth, as people seek employment opportunities, education, and access to what are often assumed to be better quality services.
Many urban migrants find themselves settled on the periphery of cities and towns – both physically and socially – where they face precarious living conditions, limited healthcare access, legal and administrative barriers, and, in many cases, xenophobic and vigilante violence. Health outcomes are shaped by intersecting factors: poverty, housing insecurity, gender-based violence, inadequate sanitation, overcrowding, and struggling public health systems, all of which are amplified as a result of prevailing anti-foreigner sentiments that drive both structural – through political influences on legislative, policy and programme development – and interpersonal violence.
While South Africa has made significant progress in addressing major public health challenges such as HIV and TB, urban migrants often remain excluded from national health and social protection systems. Today, these ‘left-behind’ populations face further challenges as a result of the withdrawal of USAID and Pepfar funding that previously supported HIV treatment-as-prevention (TasP) services. Whilst celebrating the planned roll-out of the twice-yearly lencapavir (LEN) HIV prevention injection, it remains to be seen whether targeted uptake campaigns will reach those on the margins. The same can be said for the National Health Insurance (NHI) Act that – in spite of purporting to facilitate Universal Heath Coverage (UHC) – specifically excludes asylum seekers and undocumented migrants from accessing primary and tertiary healthcare services (apart from emergency care and treatment for notifiable diseases).

0 Comments